Radiological protection
What ionising radiation are humans exposed to?
People are continuously exposed to ionising radiation, and have been so since the dawn of mankind. Some of these radiations come from nature, without human intervention in their production; others originate from human-induced actions.
The former constitutes the natural radioactive background. We can distinguish three causes of this radioactive background:
- Ionising radiation from outer space (cosmic radiation). They originate from nuclear processes taking place outside the Earth. Since the atmosphere partially absorbs radiation, the natural background due to this cause varies with altitude, so it is lower at sea level than at the top of a mountain.
- Radiation is emitted by radioactive substances in the Earth's crust. This component of the radioactive background varies considerably from one point on the Earth to another, as the distribution of chemical elements is not uniform. For example, the terrestrial radioactive background of the Sierra de Guadarrama, whose granitic rocks have a relatively high radioactivity, is much higher than that of calcareous areas.
- Radiation from radioactive isotopes contained in the human body itself, mainly carbon and potassium isotopes. To this must be added the radiation produced by the radon we inhale when we breathe, which comes from the decay of radium and thorium.
On average, 15% of the natural background dose received by a person in Spain is due to cosmic radiation; 20% to terrestrial radiation, 15% to the body itself, and 50% to radon.
The artificial causes of radiation are due to exposure to various sources of non-natural origin, such as radiological examinations for medical purposes, luminous watch dials, colour television, air travel (in this case due to the higher dose of cosmic radiation received during the flight at high altitude), the radioactive residue from nuclear explosions in the atmosphere that took place in the past, emissions from coal-fired power stations, whose fumes contain radioactive isotopes, and nuclear installations.
Among the man-made causes, the main source of radiation is radiological scans, which, in developed countries, result in doses to the population similar to cosmic radiation. Nuclear power plants produce virtually no dose to the general public, and a very small, controlled dose to plant personnel.

What are the main quantities used in radiology?
For a radioactive material, it is necessary to define in some way the ‘intensity’ with which it decays. For this purpose, the quantity called activity is used, which expresses the number of disintegrations in the material during a unit of time. In the International System of Units (SI), the unit of activity is the becquerel, whose symbol is Bq, and it is defined as the activity of a material undergoing one disintegration per second.
As the decay of a radioactive body decreases exponentially over time, its activity does not remain constant but follows the same evolution, slower or faster depending on whether it is a long- or short-lived isotope.
To study the actions of radiation on an object subjected to radiation, the quantity absorbed dose has been defined (instead of the full expression, its ellipsis, dose, is often used), which is defined as the energy transferred by the radiation to the unit mass of the irradiated material. The SI unit of absorbed dose is the gray, whose symbol is Gy. It is defined as the radiation dose that transfers an energy of 1 joule to 1 kilogram of irradiated material.
The study of the biological effects of radiation shows that these effects depend not only on the absorbed dose, but also on the type of radiation used, i.e., equal doses of two different radiations produce different biological effects. To take this into account, a new quantity, the equivalent dose, is defined, which is the product of the absorbed dose and a weighting factor for each type of radiation, to homogenise the different types of radiation from the point of view of their biological effects. This factor is 1 for X, gamma, and beta radiation; between 5 and 20 for neutrons, 5 for protons, and 20 for alpha radiation and other multiply charged particles. The SI unit of dose equivalent is the sievert, symbol Sv. It is defined as the absorbed dose of any radiation that produces the same biological effects as 1 Gy of gamma radiation.
The International System of Units was adopted relatively recently. Before this, radiological quantities were measured within a special system of units called the radiological system. It is common to find publications that still use the units of this system. Therefore, the correspondences between the units of the International System and those of the radiological system are presented below.
Units of radiological quantities in the international and radiological systems
| Magnitude | Unit and symbol (IS) | Unit and symbol (radiological protection) | Equivalence |
| Activity | becquerel (Bq) | curio (Ci) | 1 Ci = 3,7 x 10^10 Bq |
| Absorbed dose | Gray (Gy) | rad (rad or rd) | 1 rad = 10^-2 Gy |
| Equivalent dose | Sievert (Sv) | rem (rem) | 1 rem = 10^-2 Sv |
The radiological system also defined a quantity called exposure, which was used to measure the ability of radiation to produce ions in air; its unit was the roentgen (symbol R). This quantity has fallen into disuse, so its SI unit (the coulomb/kilogram) has no name. The equivalence is: 1R = 2.54 x 10^-4C/kg.
Which radiological quantities are the most significant from a radiation protection point of view?
Radiation protection is defined as the set of means employed to achieve health protection, both for the general public and for workers professionally exposed in activities related to ionising radiations, to avoid the damage that would be caused by these radiations if the doses received were sufficiently high.
Among the radiological quantities mentioned, the equivalent dose is directly related to the biological effects of radiation and should therefore be considered as the most important from the point of view of radiological protection. The regulations normally refer to this quantity when establishing the permissible limits of radiation that may be received.
When referring to the effects of radiation on a living organism, it is not only the equivalent dose that must be considered, but also the organ that receives it, since it is not the same to irradiate one or another organ of the body or to irradiate the whole organism. For this purpose, the concept of effective dose is used to establish risk values that are independent of whether the whole organism has been irradiated uniformly or, on the contrary, there has been no such uniformity. This dose is the weighted sum of the equivalent doses received by each of the tissues, according to appropriate weighting factors. It is measured in Sv.
It should be borne in mind that the successive doses absorbed by a person over time add up in terms of their effects. For this reason, the regulations refer to the committed dose as the sum of all the doses received by a person throughout his or her lifetime up to the time considered. This criterion of dose accumulation is conservative, like all those applied in radiological protection, since it disregards the possibility of the organism partially recovering from doses absorbed in the distant past. It is measured in Sv-years.
Finally, the collective dose is defined as the doses received by a group and is measured in Sv-person.
What doses do people normally receive?
Human beings are subjected to radiation from the natural background as well as from the background resulting from human activities.
Natural radiation is due to three causes: cosmic radiation, radioactive elements contained in the earth's crust, and radioactive isotopes present in the individual's own body. The dose received from this natural background varies greatly from one part of the Earth to another.
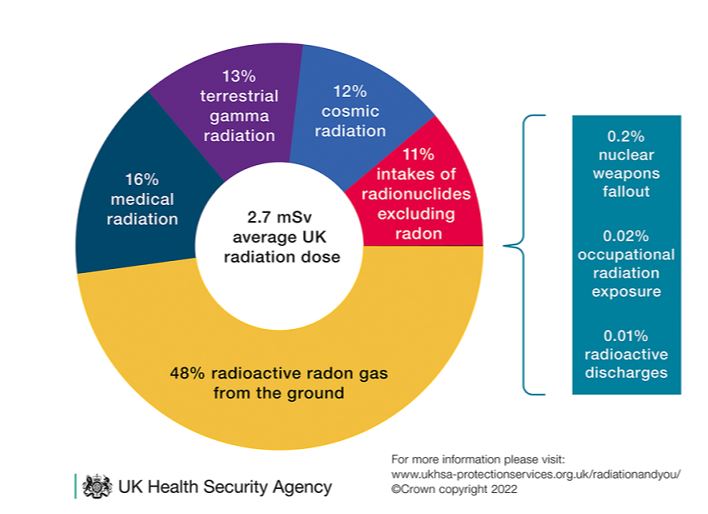
According to a report submitted by the Nuclear Safety Council to Congress and the Senate, the average dose received by a person from natural causes is 2.41 mSv/year. This dose is distributed approximately as follows: 0.35 mSv/year from cosmic radiation, 0.45 mSv/year from ground radiation, 1.26 mSv/year from the inhalation of radon, 0.34 mSv/year from isotopes incorporated into the body, and 0.01 mSv/year from the radioactive residue of nuclear experiments.
It should be noted that the large differences in the natural background between different regions of the Earth do not seem to affect the incidence of cancer, genetic defects, etc., which is a significant fact when studying the effects of radiation on people.
The dose received as a result of human activities depends to a large extent on the vicissitudes people go through. For example, a person travelling 25,000 km per year by plane would receive 1 mSv more than a person with the same lifestyle who never flies. Among all such sources of irradiation, the most important is the contribution due to radiological examinations for medical purposes, which varies considerably between individuals: in a chest X-ray, a dose of 0.05 mSv is received; in a CT scan of the lumbar region, the dose is 6 mSv.
Concerning the dose received as a result of the presence of nuclear power plants, a person remaining all year round at a distance of less than 2 km from the plant would receive an additional dose of 0.005 mSv/year; the dose would decrease as the person moved away from the plant, such that if he remained at a distance of more than 10 km he would not receive any additional dose. It should be remembered that the regulations establish areas of prohibited or restricted access in the vicinity of a nuclear power plant, so that the dose received by the general public as a result may be considered to be zero.
Are ionising radiations dangerous to living beings?
The answer to such a simple and categorical question cannot be reduced to YES or NO, without further distinction, but requires a more detailed answer.
Radiation can be used to produce a beneficial effect on people: X and gamma radiation are used for curative or palliative effects in the treatment of tumours in the technique known as radiotherapy; also, in medicine, X-radiation or radioactive isotopes are used for diagnostic purposes in the specialties of radiology and nuclear medicine. Other examples of biological uses of radiation, which are not related to human health but to human well-being, can be cited, such as the induction of genetic mutations in cereals to improve crop yields or the quality of the proteins contained in the grain.
However, radiation can cause harm or pose risks to living beings, although here again it should be noted that the effects produced by radiation depend on the doses received. With very high doses, the individual dies; with lower but still high doses, the higher the dose, the more serious the injuries; low doses do not necessarily cause damage, but rather increase the probability of the damage occurring, depending on the dose received.
For this reason, and apart from specific cases where radiation is deliberately used to produce a particular beneficial effect, radiation is considered by regulation to be potentially hazardous and should be guarded against.
What are the biological effects of ionising radiation?
Exposure of living beings to ionising radiation produces various biological effects as a result of the absorption of radiation energy by the living being. The changes produced can be studied at the cellular, organ, or tissue level, or the level of the organism as a whole.
Ionisations and excitations occur in the cell, with the formation of free radical ions, which give rise to chemical reactions that cause alterations in the functioning of the cell. These alterations, depending on the dose received, can lead to failures or delays in cell reproduction or even cell death. The sensitivity of cells to radiation varies greatly depending on the type of cell; it is much greater in less differentiated cells with a greater capacity for cell division and also depends on the moment in the cell cycle at which the irradiation occurs, with the cell being more radiosensitive in the division phases compared to those of cellular rest.
If we consider the effects of radiation on an organ or tissue, they will be related to the type of cell population that makes up the tissue; the health effects on the individual will also depend on the physiological role played by the organ or tissue. Critical organs are those that are most affected by radiation and result in the most severe consequences for the organism. The main critical organs are: the bone marrow, where blood cells are produced; the small intestine, where the processes of digestion and absorption of food take place; and the gonads, where germ cells are produced and mature.
The effects of the absorption of a large dose of radiation by the body as a whole are called irradiation syndrome, the clinical manifestations of which are a function of the doses received and reflect the damage to the bone marrow, the intestine, and the central nervous system.
How are the biological effects of radiation classified?
The biological effects of radiation can be classified according to different criteria. The three most commonly used are the classification concerning the cause-effect relationship between the radiation received and the damage it causes; the temporal relationship between the time of irradiation and the time it takes for the lesions to manifest themselves; and, finally, the appearance of the effects in the individual who received the radiation or in his or her descendants.
Under the first criterion, effects are classified as causal (or deterministic) and random (or stochastic). In causal effects, the greater the dose received, the greater the severity of injury; below a minimum dose or threshold, no injury occurs. Generally, these effects are produced by high doses of radiation that affect the tissues most sensitive to radiation and with a rapid turnover, such as the bone marrow, the digestive system, the skin, the testicles, and the ovaries.
Random biological effects are also called stochastic. They are characterised by the fact that the probability of occurrence of the biological effect depends on the dose and not on the severity, as in the previous case. They are ‘all-or-none’ effects that only occur in some individuals who receive the same dose of radiation. These probabilistic effects probably lack a minimum or threshold dose; in doubt and as a further precaution, the regulation assumes that there is no such threshold dose. Therefore, a minimal radiation dose could produce them by acting on an important part of the cell, such as deoxyribonucleic acid (DNA), causing a serious alteration.
Random or stochastic effects, if they occur, are always serious and include the possible appearance of malignant tumours such as leukaemia, lung cancer, skin cancer, etc., and genetic alterations such as hereditary anomalies.
Under the second criterion, the effects are classified as immediate (also called early or acute), which appear within a few hours to a few weeks after radiation exposure, and delayed, which appear a few years after radiation exposure.
Finally, the effects can be divided into somatic, when the damage manifests itself in the individual who has received the radiation; and genetic, when it results in lesions in their reproductive cells, so that alterations may appear in their offspring.
What are the biological effects of high radiation doses?
High doses of radiation produce immediate or early causal effects. When the dose is very high, above 100 Gy, the individual dies within a short time, between a few hours and a few days, due to the lesions produced in the central nervous system.
If the dose is between 10 Gy and 50 Gy, death occurs between one and two weeks after irradiation, due to gastrointestinal lesions.
Doses between 3 Gy and 5 Gy mainly affect the bone marrow, the producer of blood cells, which can lead to the death of half of the irradiated persons within one to two months.
At lower doses, alterations occur in various organs and tissues, which are then followed by repair and healing, leading to full or partial recovery.
Moderate irradiation of the skin with low penetrating radiation causes redness with inflammation, or erythema, which may be followed by ulceration if the doses are somewhat higher.
The genital organs are particularly sensitive to radiation: doses of 2 Gy to the testicles can produce definite sterility, and doses of 0.1 Gy can produce temporary sterility; the ovary is somewhat less sensitive, so sterility does not occur at doses of less than 3 Gy.
In the structure of the eyeball, the crystalline lens is more sensitive to radiation and may opacify to produce cataracts, which may progress to blindness. The foetus is particularly vulnerable to radiation due to the immaturity of its tissues, and precautions must therefore be taken to avoid possible exposure in pregnant women.
What biological effects occur with low doses of radiation?
The study of the biological effects of low doses of radiation is of great interest because humans are continuously exposed to natural radiation, as well as human-made radiation from medical uses, nuclear explosions, and industrial and energy applications of nuclear energy. Additionally, a portion of the public, known as professionally exposed personnel, is subjected to low doses of additional radiation due to their work over very long periods of their working life.
The first problem in studying the effects of low-dose radiation is that, given its very small incidence, it can be encompassed or masked by other causes different from radiation, which can much more frequently produce the same effects either isolated or simultaneously. Furthermore, due to this low incidence, from a statistical methodological point of view, it would be necessary to study large population samples, on the order of millions of people, for the results to be significant and to do so over several generations, as these effects can occur many years after exposure. A comparative control population not exposed to radiation, with the same environmental effects, must also be considered.
The possible biological effects of low-dose radiation are carcinogenic and genetic. Given the difficulties mentioned for studying them, different models have been produced based on extrapolating data obtained from the effects produced at high doses of exposure, assuming that there is no threshold below which effects do not occur. Some authors accept supra- or sub-linear hypotheses, according to which these effects would be respectively somewhat higher or lower than those of the linear theory. According to a 1980 United Nations expert report, in practice, with very low doses of radiation, the real risk is 2 to 10 times lower than calculated from the linear hypothesis. However, as a precautionary measure, radiological protection adopts the criterion of the least favorable linear hypothesis, as it is the most prudent.
Regarding carcinogenic effects, although the hypothesis of the absence of a threshold is theoretically established, at low doses, below 0.5 Gy, no increase in cancer incidence has been proven as a result of them, which does not mean it cannot exist, but that in the current state of epidemiological research it is not demonstrable. Studies have been extensive and varied, having been conducted on uranium miners subjected to high radon contamination, survivors of Hiroshima and Nagasaki, patients treated with radioactive iodine for thyroid cancer, etc.
In the case of genetic effects, demonstrating the possible effect of exposure to low doses of radiation is also difficult, since in the case of cancer it must be considered that 22% of the population dies from this cause, genetic defects occur spontaneously between 6% and 10% of newborns, although most of them are of minimal importance. In practice, no increase in the incidence of hereditary alterations has been observed in the descendants of people exposed to relatively high levels of radiation, as is the case in the study conducted on the descendants of American radiologists when the equipment had poor radioprotection, or in children and grandchildren of patients irradiated due to malignant tumors.
It is advisable to place the risks of low-dose ionizing radiation about other risks of daily life, as all human activity carries a risk, however small. In a comparative study carried out in France, it has been seen that the risk corresponding to the maximum allowable exposure dose of half a day in a nuclear power plant or a three-year stay near it is the same as smoking a cigarette, traveling 650 km by plane or 100 km by car, or drinking half a bottle of wine. This, which may seem anecdotal, means that the evaluation of a real risk must be done not only in qualitative terms but also quantitatively, calculating the true magnitude of it about other risks in life.
What is the difference between irradiation and radioactive contamination?
The term irradiation or exposure refers to the action of subjecting a person or object to ionizing radiation. External irradiation occurs when the radiation source is outside the individual, while internal irradiation is caused by radioactive sources located inside the individual. When both types of sources exist simultaneously, the total exposure is the sum of the two partial exposures. If the entire organism is irradiated, it is referred to as global exposure, while partial exposure refers to the irradiation of a specific organ.
Contamination is the unwanted presence of radioactive substances on the surface or inside a body or organism. External contamination occurs when radioactive substances are deposited on the skin, while internal contamination occurs when radioactive isotopes enter the organism, either by ingestion, inhalation, or through wounds etc.
An individual irradiated by a radioactive source outside of them experiences the biological effects of radiation in their tissues while they are near the source, but simply moving away from it will stop the irradiation. Conversely, a contaminated individual will continue to be irradiated as long as the contamination persists, and they can act as a source of contamination or irradiation to other people.
External contamination is easily removable by washing the contaminated surface, while the effects of internal contamination depend on the tropism of the radioactive elements, which causes them to deposit in various organs based on their metabolic characteristics. The duration of the action of radionuclides depends, on one hand, on the organism's ability to eliminate the substance through natural pathways, and on the other hand, on the half-life of the isotope in question.
What is radiological protection, and what are its objectives?
The misuse of ionizing radiation can be dangerous for living beings, so in any activity where irradiation from a radiation source or radioactive contamination can occur, it is necessary to ensure that people and other living beings are protected from receiving a dose that could pose radioactive risks.
Radiological protection is concerned with this, defined as the set of regulations, methods, and actions taken to avoid these risks and damages, as well as the actions, measures, and analyses carried out to verify that the appropriate protection criteria have been correctly applied. In a nuclear or radioactive facility, there is at least a theoretical possibility that radioactive products may be emitted into the environment, which could then harm living beings; therefore, radiological protection also establishes limits on radioactive emissions to the environment and measures the radioactivity in it.
Radiological protection did not originate with nuclear power plants; rather, when it was found that the improper use of radiation is dangerous, the first protection standards against X-rays were established in 1901, and the first recommendations on protection against X-rays and radium were made in 1916. During the first four decades of the 20th century, ionizing radiation was used only in medicine, so radiological protection was concerned only with the medical uses of radiation.
When nuclear energy applications were developed in the mid-20th century, radiological protection also began to address nuclear issues and gained the prominence and importance it has today.
Which international organizations are involved in radiological protection?
The oldest among them is the International Commission on Radiological Protection (ICRP), established in 1928 under the name International Commission for Protection against X-rays and Radium, a name that indicates its focus on medical applications of radiation. Originally, it was composed only of doctors and biologists, but when its scope expanded to include radiological protection of nuclear and radioactive facilities in 1950, it changed its name and incorporated physicists, chemists, engineers, etc.
It has four committees dedicated to:
- Radiation effects.
- Definition of secondary limits of body burden.
- Radiological protection in medicine.
- Implementation of its recommendations.
Although this Commission is not intergovernmental, its prestige and the scientific solidity of its recommendations make them accepted by all international organizations and adopted by the official regulations of all states that develop nuclear activities.
The most important intergovernmental nuclear organization in the world is the International Atomic Energy Agency (IAEA), created by the United Nations in 1956. The Agency's headquarters are in Vienna, and it has 140 member states as of March 2006. Its tasks are very broad within the field of nuclear energy, such as research and development, holding scientific conferences, monitoring the peaceful uses of fissile materials, and formulating recommendations on nuclear safety and radiological protection. Spanish regulations require that these IAEA recommendations, like those of other international organizations of which Spain is a member, be mandatory in Spanish nuclear and radioactive facilities.
The Nuclear Energy Agency (NEA) of the OECD was created within the Organization for Economic Cooperation and Development in 1957. It includes 22 European states, as well as Canada, the United States, Japan, Australia, Korea, and Mexico; its headquarters are in Paris. Within the Agency, there are four technical directorates: nuclear sciences and techniques; technological development; nuclear safety; radiological protection and radioactive waste management. As Spain is a member of the NEA, its recommendations, like those of the IAEA, are mandatory in Spain.
The European Atomic Energy Community (EURATOM), now integrated within the European Union, also establishes regulations on radiological protection, which are required of Union member states.
Other international organizations make recommendations on radiological protection. The most important ones include: the World Health Organization (WHO), the International Labour Organization (ILO), and the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR).
Which organization is responsible for radiological protection in Spain?
When nuclear research began in Spain in 1948, the Nuclear Energy Board was tasked with overseeing the country's radiological protection.
As had happened in other nations, given the rise of nuclear energy, in 1980, it was decided to create an organization dedicated exclusively to nuclear safety and radiological protection, which would operate independently of other public administrations.
To this end, Law 15/1980, of April 22, created the Nuclear Safety Council as a "Public Law Entity, with legal personality and its own assets independent of those of the State, and as the sole competent body in nuclear safety and radiological protection." The Council is governed by a president and four councilors, "appointed from among persons of recognized expertise in the fields of nuclear safety, technology, radiological and environmental protection, medicine, legislation, or any other related fields, as well as in energy in general or industrial safety, with special emphasis on their independence and objectivity of judgment," and it has its own body of officials, the Technical Corps of nuclear safety and radiological protection.
Radiological protection has been a concern of the State since the very beginning of nuclear activities in Spain, and therefore, there is a capable and independent technical body that ensures the protection of people and the environment from ionizing radiation.
How can people protect themselves from irradiation by an external source?
When a person is subjected to irradiation from an external source, the radiation dose received is equal to the product of the dose rate (dose received per unit of time) by the time during which they are exposed to the radiation.
The dose rate at a point is proportional to the radiation flux at that point, and this flux decreases with distance from the radiation source according to the product of two factors: the first follows the inverse square law; that is, even if the radiation is not absorbed on its way from the source to the irradiated object, the dose rate would decrease inversely proportional to the square of the distance from the emitting source, in the case of a point source.
Additionally, radioactivity is partially absorbed by the medium between the emitter and the receiver, meaning that the second factor of dose rate decreases with distance,e follows an exponential law.
As a result, protection against irradiation from an external source is achieved through the combination of three factors: exposure time, distance, and shielding.
Exposure time should be minimized so that the person remains in the irradiation zone for the shortest necessary period, and the time spent in that zone should be controlled.
The distance between the source and the person should also be controlled, ensuring that they are as far away from the source as possible.
Since it is not always possible for the combination of exposure time and distance to result in an acceptable dose, protection is achieved by interposing a substance that absorbs the radiation between the source and the subject. This is known as radiation shielding.
- Alpha radiation is easily absorbed by all bodies: a few centimeters of air or a few hundredths of a millimeter of water are sufficient, so protection against alpha radiation does not require any shielding.
- Beta radiation, although somewhat more penetrating, is also easily absorbed, requiring only a few meters of air, a few millimeters of water, or a thin solid.
- On the other hand, gamma radiation is very penetrating, so to protect against it, thick shields of heavy material, such as lead or concrete, are necessary.
- Neutrons are also very penetrating and are not absorbed by air. Compounds of certain chemical elements, such as boron and cadmium, are good neutron absorbers.
- In nuclear power plants, the reactor is surrounded by strong shielding that absorbs much of the gamma radiation and neutrons, and the plant is divided into areas according to the radiation levels present. Access to the interior of areas with appreciable radiation levels is strictly controlled and only allowed for personnel performing specific tasks; their time in the zone is limited, and the dose received is measured, which must never exceed the limits authorized by regulations. Outside the plant, as well as in the office and rest areas, the radiation level is zero.
What measures are used for radioactive decontamination of people?
As a consequence of nuclear accidents or explosions, irradiation and contamination of people can occur. In order not to act impulsively, it is necessary to have a series of actions planned and foreseen. If people require first aid resuscitation or emergency treatment, these will take precedence over decontamination measures. It is essential to try to know from the first moment which radionuclides are contaminating as well as their physical and chemical forms, as this will facilitate the actions of healthcare personnel.
In the case of external contamination, the procedure followed is aimed at eliminating it and preventing it from being incorporated into the body through wounds, natural orifices, or inhalation, in the case of contaminated atmospheres. The measures consist of removing clothing, storing it in plastic bags; showering with warm water and neutral soap, in the case of diffuse contamination, or simply washing the contaminated areas, in the case of defined areas. Washing and rinsing are repeated as many times as necessary, controlling with a detector that the decontamination is as perfect as possible. In the case of wounds and to prevent the incorporation of contaminating agents through lymphatic and blood vessels, it is advisable to compress the veins near the wounds and wash them with physiological saline, applying antiseptics and sterile dressings.
Internal decontamination measures are more complex and are related to the metabolic characteristics and diffusion capacity of the radioisotope, its physical characteristics (activity, energy, half-life), as well as the route of entry and special tropism for certain organs. For example, we know that radioactive iodine accesses the thyroid, cesium the muscle, strontium the bones, etc. The first measures taken tend to favor the elimination of radionuclides, for which the contaminated person is made to drink plenty of fluids or mild laxatives, bronchial fluidifiers, etc., as well as appropriate medications to try to form chemical complexes with the radionuclides, or to block their uptake by critical organs.
What are the basic principles on which radiological protection is based?
Ionizing radiation is not always harmful to people's health, and in certain cases, such as medical applications of radiation, it can be beneficial. But given the possibility that radiation may cause damage, depending on the circumstances, or involve a risk of damage occurring, it is universally accepted that, outside of therapeutic applications, ionizing radiation should always be considered potentially dangerous.
Consequently, no one should ever receive a dose that is not necessary; the dose must always be below established limits, which are known to be non-dangerous; the dose, even below these limits, must always be the minimum possible; in the case that a person performs an activity in which they may receive doses above the natural background, the dose must be controlled and measured.
What are the radiological protection regulations established by the legislation?
Spanish regulations establish the maximum doses that, under no circumstances, can be exceeded. The regulations distinguish between members of the public, who are people not engaged in activities specifically related to radiation (i.e., the "ordinary citizen"), and professionally exposed personnel, who are people working in nuclear activities, who have received special training to perform these tasks and are subject to strict medical and radiological control.
Additionally, for radioactive isotopes, there are limits on the admissible body burden; that is, the maximum amount of each isotope that can be incorporated into the body.
The maximum dose values and admissible body burden set by Spanish regulations are the same as those established in other national regulations and recommended by international organizations.
Due to the development of scientific knowledge related to radiological protection, the ICRP in its publication No. 60 (1990) recommended the modification of the limits. This recommendation has been adopted by EURATOM, which issued Directive 96/29, so that the new limits came into force in the member countries of the European Union in May 2000.
a) For professionally exposed personnel:
- Annual effective dose limit: 20 mSv (100 mSv in 5 years)
- Annual dose limits to the lens of the eye: 150 mSv
- Annual dose limit for the skin: 500 mSv
- Annual dose limit for the hands, forearms, feet, and ankles: 500 mSv
b) Dose limits for students who are going to pursue a profession involving exposure to ionizing radiation or who must handle sources due to their studies:
- If they are 18 years or older, the limit is the same as in section a).
- If they are between 16 and 18 years old, the limits are 3/10 of those in section a).
c) Dose limits for the general public:
- Annual effective dose limit: 1 mSv
- Annual dose limit to the lens of the eye: 15 mSv
- Annual dose limit for the skin: 50 mSv
- Annual dose limit for the hands, feet, and ankles: 50 mSv
Limits are also established for planned special operations, as well as special conditions for pregnant women, breastfeeding mothers, apprentices, and students.
What are the radiological protection measures adopted in a nuclear power plant and its surroundings?
These measures aim to ensure that no unauthorized contamination or discharges of radioactive products occur and that the radiation dose received by people is below the limits established in the regulations.
To achieve this, the plant is designed and constructed in such a way that radioactive products are confined, meaning that contamination is prevented; discharges of small amounts to the outside must be below limits that have been previously calculated, taking into account the characteristics of the environment, so that they do not pose the slightest risk. These limits are approved by the Nuclear Safety Council. Additionally, the project studied what shielding needs to be placed to reduce radiation levels within the plant, to allow necessary work to be carried out within the facility.
Before the plant is put into operation, an operation regulation is drafted that, according to the maximum radiation levels that can be reached in the different areas of the plant, divides it into zones, according to the maximum time of stay in them: in the permanent access zone, the radiation level is zero; there are various classes of controlled zones, according to their radiation levels, where it is limited who and for how long they can stay and the precautions that must be observed.
During the operation of the plant, radiation and contamination levels are measured in the various zones to ensure they are following what was planned. The radiological protection service ensures that personnel comply with the established regulations and measures the doses received by people, and in the event of deviations from what was planned in the regulations, decides the measures to be taken.
Regarding the surroundings, two years before any radioactive material is introduced into the plant, a systematic control of environmental radioactivity (air, rivers, sea, fauna, flora, crops, etc.) is carried out to know the background radioactivity of the region. During the operation of the plant, these measures continue, and the slightest deviation above the admitted limits would lead to the immediate shutdown of the plant.


